28 year old male with pedal edema and SOB
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case presentation:28 year old male who is a coal worker came with chief complaints of palpitations followed by SOB since 1 week and pedal edema since 4 days.
Apparently normal 1yr back, developed symptoms of neck pain and giddiness,so he consulted a local doctor and he was diagnosed with hypertension with bp-160/100mmhg for which he used the medications given by the doctor for two days and discontinued the medications as the bp was recorded normal as advised by his doctor.
He came to our OPD with complaints of-Palpitations sudden in onset , no aggrevating and releving factors then he developed SOB at rest (grade-4) since 7 days ,gradual onset progressive in nature ,aggrevated with work later he developed pedal edema bilateral till knee sudden in onset which gradually progressed to thigh 2days, relieved on limb elevation
Past history :
h/o of hypertensive since 1yr
No h/o dm , asthmaa
No similar complaints in the past .
Family h/o:
His mother is known case of diabetic , hypertensive and hlo of stroke ( paraplegia)
Personal h/o :sleep adequate
Diet mixed
Addictions : Regular intake of 180 ml whiskey since 1 nd 1/2 year
On examination -
Pt is c/c/c
There are no signs of pallor ,icterus ,cyanosis ,clubbing,
Bilateral pitting type of pedal edema is present upto groin region

His vitals : afebrile
Bp - 160/70 mmHg
Pulse - 90 BPM
RR - 22cpm
GRBS - 117 mg %
Spo2 - 96%
Jvp raised
Systemic :
P/A :
Shape of abdomen : obese
no scars , sinuses ,no distended veins ,hernial orifices free ,soft
No tenderness
RS :nvbs heard
No added sounds
CNS : NAD
CVS :
S1 S2 heard
S3 gallop present
Parasternalheave
JVP raised above the angle of mandible
Day1-
Investigations ordered :
HEMOGRAM :

RFT:

LFT:

USG ABDOMEN:

CUE:

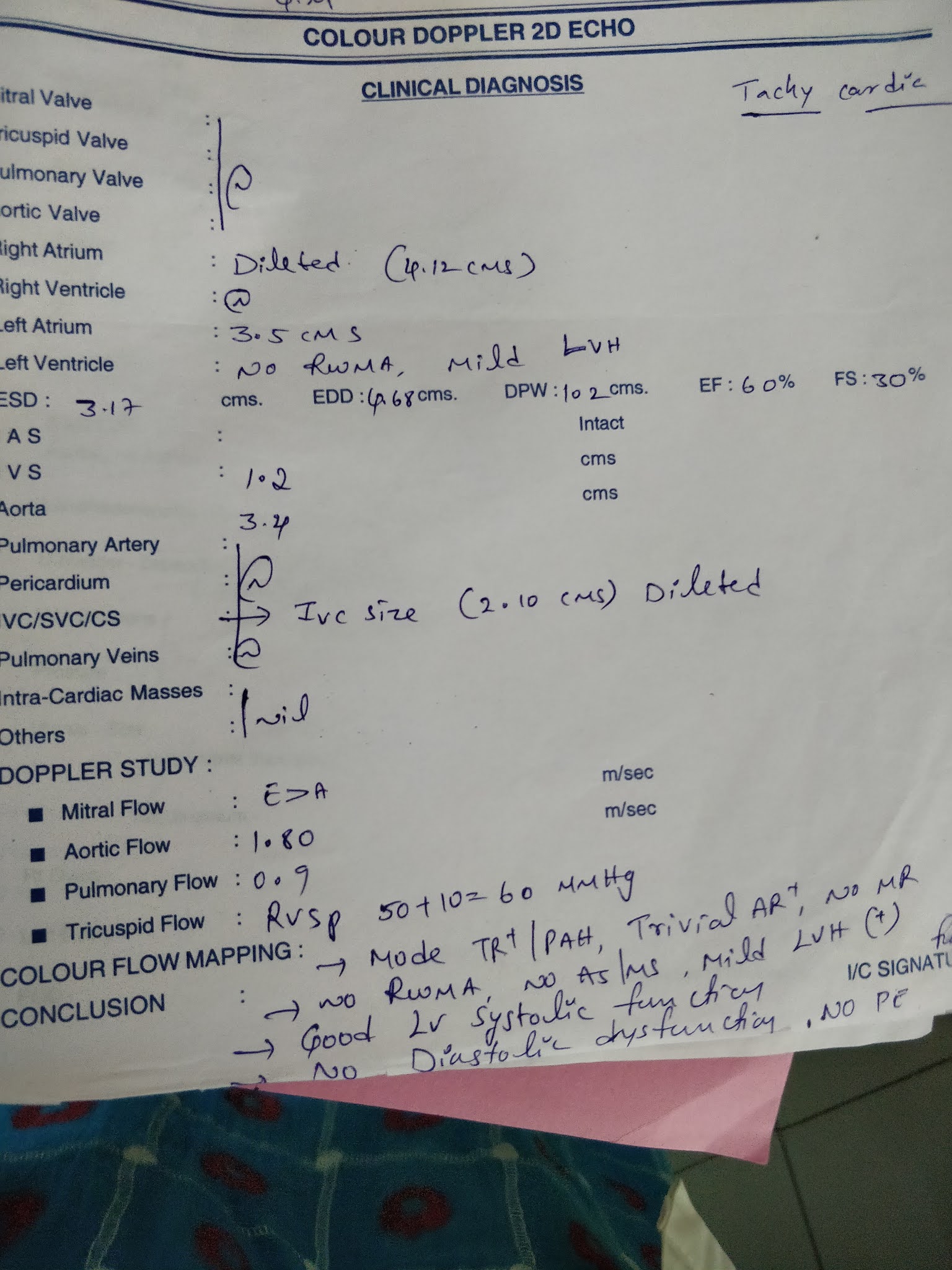
2D ECHO :
CHEST X RAY :

Treatment given :
PROPPED UP POSITION
INJ PANTOP 40 MG /IV / OD
INJ LASIX 40 MG /IV / TID
I/O CHARTING
DAILY WEIGHT MONITORING
BP/ PR HOURLYProvisional diagnosis on admission:
Heart failure with preserved ejection fraction (EF -60%)
Day 2-
No fresh complaints
Orthopnea - decreased
PND -decreased
SOB - decreased
O/E :
Patient is C/C/C well oriented to time , place , person
Pallor +
No signs of icterus ,cyanosis , clubbing,
Lymphadenopathy, edema
Vitals : afebrile
BP - 160/80 mmhg
PR - 97 bpm
GRBS - 123 mg %
Weight : 74 kg
Fever - absent
I/O - 400/2800ml
CVS - loud S1 , parasternal heave present pansystolic in tricuspid area .
RS - BAE +
P/A - soft , non tender
CNS - NFND
Investigations
ECG

Treatment given:
PROPPED UP POSITION
INJ PANTOP 40 MG /IV / OD
INJ LASIX 40 MG /IV / TID
I/O CHARTING
MAINTAIN SPO2 more than 95%
DAILY WEIGHT MONITORING
BP/ PR HOURLY
FLUID RESTRICTION less than 1 lit /day , salt restriction less than 2gm / day
TAB ECOSPRIN 75 MG OD
TAB ALDACTONE 50MG OD
INJ THIAMINE 100MG /IV / BD
Diagnosis-
Heart failure with preserved ejection fraction
Day 3
No fresh complaints
O/E :
Patient is C/C/C well oriented to time , place , person
Pallor +
Edema +
No signs of icterus ,cyanosis , clubbing,
Lymphadenopathy
Fever - absent
Weight - 73 kg
I/O - 700/900
Stools - passed
Vitals : afebrile
BP - 150/120 mmhg
PR - 103 bpm
GRBS - 112mg %
Weight : 74 kg
CVS - S1 ,S2 + ,S3 in tricuspid area parasternal heave
RS - BAE +
P/A - soft , non tender.
CNS - NFND
Treatment given:
PROPPED UP POSITION
INJ PANTOP 40 MG /IV / OD
INJ LASIX 40 MG /IV / TID
INJ THIAMINE 100MG /IV / BD
TAB ATORVAS 20 MG H/S
I/O CHARTING
MAINTAIN SPO2 more than 95%
DAILY WEIGHT MONITORING
BP/ PR HOURLY
FLUID RESTRICTION less than 1 nd half lit /day , salt restriction less than 2gm / day
TAB ECOSPRIN 75 MG OD
TAB ALDACTONE 50MG OD
TAB RAMIPRILL 5NG OD - 8AM
Diagnosis : Heart failure with preserved ejection fraction with denovo
Comments
Post a Comment