A 54 year old with chest pain
A 54 year old Toddy tree climber came to opd with chief complaints of
1. Swelling of both the legs since 15 days
2. chest pain since 10days
3. Facial puffiness since 10days
4. Difficulty in breathing since 7days
Patient was apparently asymptomatic 15days back then he developed bilateral pitting type of pedal edema extending Upto knees. He had on and off symptoms of Chest discomfort and pain since 10days. He also developed facial puffiness 10 days back which temporarily relieved with medication and often reappears. Since 7 days he has grade 2 shortness of breath.
No H/o palpitations, orthopnea, PND.
No H/o fever, cough. Urine output is normal.
No H/o pain abdomen/ vomitings / burning micturition.
Past History:
Not a k/c/o DM, Hypertension, Tuberculosis, Asthma, Epilepsy
No similar complaints in the past.
His mother was hypertensive.
Personal History:
He takes mixed diet
Appetite normal
Adequate sleep
Addictions: Alcoholic since 40 years (90ml of liquor/day)
Smoked beedis 18/day since 40 years.
Vitals:
Temp: 98.4F
Pulse: 92bpm, regular rhythm, normal volume and character, no radio-radial and no
radio-femoral delay.
BP: 180/100mmhg measured on right arm in sitting position
RR: 18cpm
SpO2: 98% on room air
General Examination:
Pallor, Icterus, Cyanosis, Clubbing, Lymphadenopathy are absent.
Bilateral pitting type of pedal edema is present upto knees.
Systemic examination:
CVS:
On inspection:
JVP raised.
Apical impulse seen in 6th intercostal space.
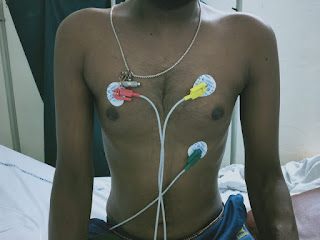
Pectus excavatum is present

Trachea central.


On palpation:
All inspection findings are confirmed.
Apex beat shifted to 6th intercostal space midclavicular line
No pulsations, palpable sounds or thrills felt in mitral, tricuspid, aortic and pulmonary areas.
On auscultation:
S1, S2 heard. No murmurs
Respiratory: BLAE, Normal vesicular breath sounds heard.
CNS: No focal neurological deficit.
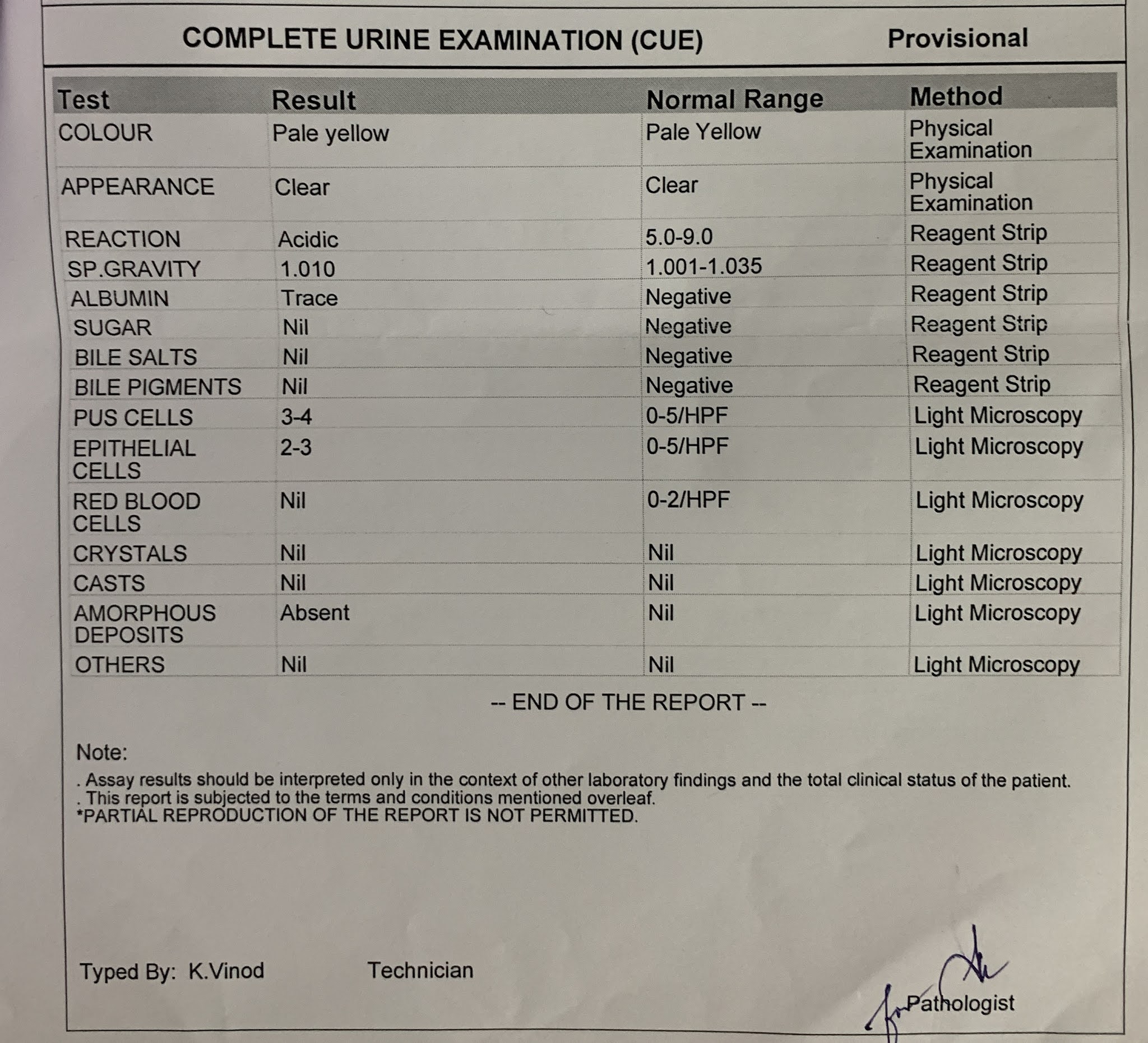
INVESTIGATIONS:




TREATMENT:
1. Inj. LASIX 20mg IV BD
2. Tab. MVT PO OD
3. Tab. PANTOP 40mg IV OD
4. Tab. THIAMINE 100mg po TID
5. Tab. TELMA 20mg OD
6. Tab. SPIRINOLACTONE 25mg po OD


Comments
Post a Comment