SHORT CASE-2
A 55-year-old male, resident of Nalgonda, who is a farmer by occupation came to the hospital with chief complaints of breathlessness since 6 months
• HOPI :
Patient was apparently asymptomatic for 20 years then had muscle cramps, increased frequency of urination, and giddiness for which he went to hospital and was diagnosed with DM type II and is on medication (T.Glymiperide + Metformin) since then.
1 year back he had generalized weakness, polydipsia, polyurea, and dizziness, visited the hospital and was found to have uncontrolled DM 2 and is on insulin ( since then.
Until 6 months ago he worked as a farmer, waking up at 5 am. he takes his breakfast at 7 am. Then he goes to work, has lunch at 1 pm. returns to home at 6-7 pm & has dinner at 8 pm, and goes to bed at 9 pm.
But 6 months back his whole life was changed when he was taken to the hospital after experiencing palpitations, dizziness, blurring of vision, and involuntary movements involving his upper limbs & body, where he was diagnosed with hypertension & Renal failure.
H/o SOB since 6 months NYHA 1-2 and from last 1-month shortness of breath increased NYHA 3-4, gradually progressive, associated with orthopnea & PND for which he came to our hospital.
H/o Low backache since 1 month
H/o itching all over the body with darkening of skin since 1 month
H/o decreased Urine output since 1 month
No thin stream, poor flow, increased frequency, hesitancy, or Burning micturition present.
No h/o Fever, Chest pain, Palpitations, Syncope
No h/o Cough
No other complaints
•Past History :
K/c/o DM-type II since 20 years
K/c/o hypertension since 6 months
No history of asthma, TB, epilepsy, thyroid abnormalities
•PERSONAL HISTORY:
Diet: Mixed
Appetite: Normal
Sleep: Disturbed
Bowel: Regular
Bladder: Decreased urination.
Habits: Do not consume any form of alcohol or tobacco.
●FAMILY HISTORY:
Not significant
●DRUG HISTORY:
HAI & NPH 3 units (three times a day) Insulin for the past 1 year,
TELMA for hypertension since the past 6 months
●GENERAL EXAMINATION:
The patient was examined in a well-lit room after obtaining consent.
The patient was conscious, coherent, and cooperative. He was moderately built and moderately nourished.
Pallor: Absent
Icterus: Absent
Cyanosis: Absent
Clubbing: Absent
Generalized Lymphadenopathy: Absent
Pedal Edema: Absent
.jpg)
.jpg)
.jpg)
.jpg)






Vitals :
Temperature - Afebrile
BP - 130/80 mm Hg
Pulse - 78 BPM
RR - 24 CPM
Rbs - 124 mg/dl @ 7pm
●SYSTEMIC EXAMINATION:
Cardiovascular system:
•Inspection:
Shape of the chest appears to be elliptical & bilaterally symmetrical
Apex beat is not visible
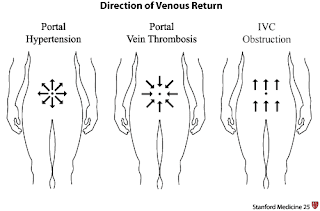
No scars, sinuses, dilated veins
No precordial bulge is seen.
•Palpation:
All inspectory findings are confirmed
Trachea is central
Apex beat felt at 6th intercostal space 1cm lateral to midclavicular line.
•Auscultation:
In Aortic, Pulmonary, Tricuspid & Mitral areas
S1 and S2 heard.
No murmurs heard
Respiratory system:
•Inspection
Shape of chest appears to be elliptical and bilaterally symmetrical.
Trachea appears to be central
No scars, sinuses, or engorged veins.
Symmetrical expansion of the chest
•Palpation:
All inspectory findings are confirmed
Trachea appears to be central
Tactile vocal fremitus normal in all areas
•Percussion:
Resonant note is heard in all areas
•Auscultation :
Normal vesicular breath sounds are heard.
No adventitious breath sounds.
ABDOMEN:
obese abdomen
Moves symmetrically with respiration
Umbilicus is central and inverted
No scars or sinuses
No local rise in temperature
No organomegaly
CNS:
Higher mental functions intact.
Motor examination:
Power: B/l Upper limbs: 4 + bilaterally
B/l Lower limbs: 4 + bilaterally.
Tone: Normal
Reflexes: R L
Biceps: 2+ 2+
Triceps: 2+ 2+
Knee: 2+ 2+
Ankle: 2+ 2+
Sensory examination: normal.
Cerebellar examination: normal.
Cranial nerve examination: normal.
Provisional diagnosis:
Acute on chronic LVF
Chronic renal failure since 6 months with?Uremic pruritis
●Investigations :
X-Ray chest

Interpretation :
Cardiomegaly
ECG

Sinus Tachycardia

• Treatment :
Fluid restriction <2L /day
Salt restriction <2g /day
INJ HAI & NPH 3Units
Tab Lasix 40 mg BD
Tab Nicardia 20 mg PO/TID
Tab Arkmain 0.1mg PO/TID
Tab Orofer -XT PO/OD
Hemodialysis

Comments
Post a Comment