Thursday, May 28, 2020
Right heart failure
Hello everyone.....!! I am an intern in medicine department and one of the important terms of getting the internship completion is to complete my log book with my daily log of what I learn during the course of my duties.
CASE PRESENTATION:
A 45year old Male labourer came to the hospital with the chief complaints of dribbling of urine since 1 week, burning micturition since 1week, shortness of breath since 1week. Anuria since 3 days.
HOPI-
- He was apparently asymptomatic 1 week back then he developed dribbling of urine associated with burning micturition without fever, low backache, suprapubic tenderness.
-Associated with B/L pedal edema upto knee of pitting type.
-Associated with shortness of breath grade 3 since 1 week progressed from grade 2 within 10 days.No h/o orthopnea and PND. No h/o palpitations, loss of consciousness,giddiness.
-C/o constipation since 1 week not associated with obstipation. C/o nausea since 1 week with burning sensation in epigastrium, associated with decreased appetite
PAST HISTORY-
-no similar complaints in the past
-patient is not a k/c/o HTN,DM,CKD,CAD,epilepsy, asthma, TB
DRUG HISTORY- not allergic to any known drugs.
FAMILY HISTORY- no similar complaints in the family
PERSONAL HISTORY:
diet-mixed
appetite-decreased
B&B- Irregular; anuria since 3 days, oliguria since 7 days ,constipation since 7days.
sleep-adequate
Addictions-alcoholic since 15 years & regular toddy drinker.
EXAMINATION-
GENERAL EXAMINATION:
Patient is conscious,coherent and cooperative.
Moderately nourished and built.
Temperature: afebrile
BP: 70/50 mm of hg measured in right arm in sitting position.
PR: 92 beats per min
RR: 28 cycles per min.
SpO2: 97% on room air
GRBS: 108mg%.
No signs of pallor, icterus, cyanosis, clubbing, kilonychia, generalised lymphadenopathy.
h/o bilateral pedal edema progressing upto knee.
RESPIRATORY SYSTEM EXAMINATION:
Dyspnoea- present [ grade 3 since 1week ]
Wheeze- no
Position of trachea- central
Breath sounds- vesicular
Adventitious sounds- no crepts and rales.
PERABDOMINAL EXAMINATION:
Shape : scaphoid, soft
no tenderness and local rise of temperature.
no palpable mass
hernial orifice : normal
no free fluid , no bruits
liver and spleen - not palpable
bowel sounds- sluggish
CNS EXAMINATION:
Higher mental functions- normal
cranial nerves- normal
motor system- normal
sensory system - normal
CARDIOVASCULAR SYSTEM EXAMINATION:
1)Pulse- 92bpm, regular, low volume, condition of vessel normal, no radioradial delay and radiofemoral delay.
2)BP- 70/50 mm of hg
3) neck veins examination: engorged
JVP raised upto bifurcation of carotid.
heart examination:
- inspection:
shape-normal
apical impulse at 5th intercostal space in midclavicular line.
no engorged superficial veins
no scars, sinuses.
no pulsations seen in other areas beyond precordium.
- Palpation:
a) mitral area:
apex beat- 5th intercostal space in mid clavicular line
no thrills.
b) pulmonary area: normal
c) aortic area: normal
d) tricuspid area: normal
-Auscutation:
cardiac rate-92bpm
rhythm-irregular
S1 S2 heard
no murmurs.
Based on the above findings, following investigations were sent
1) CBP
2) CUE
3) URINE culture and sensitivity
4) HIV, HBV, anti HCV
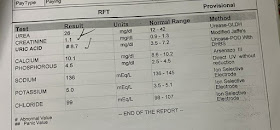
5) RFT
6) ESR
7) CXR- PA view(bedside)
8) ABG
9) 2d ECHO
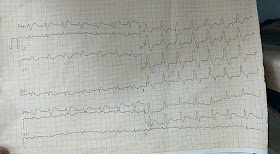
10) ECGDIAGNOSIS:
Decompensated right heart failure secondary to mild pulmonary artery hypertension. Anuria secondary to ? Bladder outlet obstruction. ? Ishaemic hepatitis. ? Cystitis. With hyperkalemia. ? Cardiorenal syndrome. With post renal AKI. With cardiogenic shock.
TREATMENT:
1) foleys catheterisation
2) salt(<2g /day) and fluid( 1.5 lts /day) restriction
3) head end elevation
4) oxygenation to maintain SpO2 > 95%
5) Inj. lasix 20mg bd if sbp> 110mmhg
6) Inj. noradrenaline 2 amp in 50 ml NS iv at 2ml/hr.
- He was apparently asymptomatic 1 week back then he developed dribbling of urine associated with burning micturition without fever, low backache, suprapubic tenderness.
-Associated with B/L pedal edema upto knee of pitting type.
-Associated with shortness of breath grade 3 since 1 week progressed from grade 2 within 10 days.No h/o orthopnea and PND. No h/o palpitations, loss of consciousness,giddiness.
-C/o constipation since 1 week not associated with obstipation. C/o nausea since 1 week with burning sensation in epigastrium, associated with decreased appetite
PAST HISTORY-
-no similar complaints in the past
-patient is not a k/c/o HTN,DM,CKD,CAD,epilepsy, asthma, TB
DRUG HISTORY- not allergic to any known drugs.
FAMILY HISTORY- no similar complaints in the family
PERSONAL HISTORY:
diet-mixed
appetite-decreased
B&B- Irregular; anuria since 3 days, oliguria since 7 days ,constipation since 7days.
sleep-adequate
Addictions-alcoholic since 15 years & regular toddy drinker.
EXAMINATION-
GENERAL EXAMINATION:
Patient is conscious,coherent and cooperative.
Moderately nourished and built.
Temperature: afebrile
BP: 70/50 mm of hg measured in right arm in sitting position.
PR: 92 beats per min
RR: 28 cycles per min.
SpO2: 97% on room air
GRBS: 108mg%.
No signs of pallor, icterus, cyanosis, clubbing, kilonychia, generalised lymphadenopathy.
h/o bilateral pedal edema progressing upto knee.
RESPIRATORY SYSTEM EXAMINATION:
Dyspnoea- present [ grade 3 since 1week ]
Wheeze- no
Position of trachea- central
Breath sounds- vesicular
Adventitious sounds- no crepts and rales.
PERABDOMINAL EXAMINATION:
Shape : scaphoid, soft
no tenderness and local rise of temperature.
no palpable mass
hernial orifice : normal
no free fluid , no bruits
liver and spleen - not palpable
bowel sounds- sluggish
CNS EXAMINATION:
Higher mental functions- normal
cranial nerves- normal
motor system- normal
sensory system - normal
CARDIOVASCULAR SYSTEM EXAMINATION:
1)Pulse- 92bpm, regular, low volume, condition of vessel normal, no radioradial delay and radiofemoral delay.
2)BP- 70/50 mm of hg
3) neck veins examination: engorged
JVP raised upto bifurcation of carotid.
heart examination:
- inspection:
shape-normal
apical impulse at 5th intercostal space in midclavicular line.
no engorged superficial veins
no scars, sinuses.
no pulsations seen in other areas beyond precordium.
- Palpation:
a) mitral area:
apex beat- 5th intercostal space in mid clavicular line
no thrills.
b) pulmonary area: normal
c) aortic area: normal
d) tricuspid area: normal
-Auscutation:
cardiac rate-92bpm
rhythm-irregular
S1 S2 heard
no murmurs.
Based on the above findings, following investigations were sent
1) CBP
2) CUE
3) URINE culture and sensitivity
4) HIV, HBV, anti HCV
5) RFT
6) ESR
7) CXR- PA view(bedside)
8) ABG
9) 2d ECHO
10) ECGDIAGNOSIS:













Decompensated right heart failure secondary to mild pulmonary artery hypertension. Anuria secondary to ? Bladder outlet obstruction. ? Ishaemic hepatitis. ? Cystitis. With hyperkalemia. ? Cardiorenal syndrome. With post renal AKI. With cardiogenic shock.
TREATMENT:
1) foleys catheterisation
2) salt(<2g /day) and fluid( 1.5 lts /day) restriction
3) head end elevation
4) oxygenation to maintain SpO2 > 95%
5) Inj. lasix 20mg bd if sbp> 110mmhg
6) Inj. noradrenaline 2 amp in 50 ml NS iv at 2ml/hr.
Patient was being monitored continuously for 14-15hrs , during which pt condition was worsened( GCS <7 , no carotid pulse) so cpr of 5 cycles done ,then pulse was restored. Pt was intubated due to falling saturation and low GCS (<3)
In some time , again the pt condition was worsened due to ventricular tachycardia so shock at 300j was given
7) infusion amiodarone
8) Inj. zofer 4mg iv tid
9) Inj. pantop 40mg iv bd
10) Tab. nodosis 500 mg p/o bd
11) syrup sucralfate 15ml p/o tid
12) syrup lactulose 15ml h/s
13) I/O charting and bp monitoring
8) Inj. zofer 4mg iv tid
9) Inj. pantop 40mg iv bd
10) Tab. nodosis 500 mg p/o bd
11) syrup sucralfate 15ml p/o tid
12) syrup lactulose 15ml h/s
13) I/O charting and bp monitoring
14) inj. Tramadol 1 amp diluted in 20ml NS slow I/v over 5 mins sos
15) neb. Salbutamol 4 respules tid
16) I/v DNS 250ml with 6 units INSULIN i/v stat
17) tab. PAH 20mg p/o tid.
Patient was shifted to higher centres with ambu bag and oxygen in ambulance upon the request of his attenders


Comments
Post a Comment