202022457
A 35 year old gentleman from South India whos' a porter by occupation presented with a 2 month history of progressive bilateral pedal oedema and swelling of the scrotum and penis.
His earliest recollection of being absolutely normal goes back to days prior to the national lockdown, when he remembers he first developed heavy bounding palpitations, which he describes, "as a ball kicking his chest from within". The palpitations were often associated with dyspnea and sweating. They were initially intermittent, associated with exertion (lifting heavy weights) and relieved with rest for a few minutes. On probing further, he also recalled that twice in the last few months, he had to wake up from his sleep, feeling breathless and sweating profusely and felt a sense of "air hunger" and a need to seek fresh air. He reports that he used to walk on the road for an hour on so at 2 in the wee hours. Over the last two months his symptoms started becoming even more bothersome, as they were only intermittent earlier. On direct questioning, he reports an insignificant chest pain and a rare nocturnal dry cough. He denies wheezing at any point. He also reported to us that the patient occasionally felt dizzy, with hollowing of vision and sweating during these episodes. He denies loss of appetite and involuntary weight loss.
On targeted review of systems, the patient reports a nagging pins and needles sensation in his feet since 1 year, which has now ascended to his fingers. He denies numbness. The patient also told us that he had slippage of footwear for the past few months, which he gets to know quite a few seconds after they have slipped. He also reported difficulty in walking in the dark since a month. He cannot quite recall a significant muscle weakness in upper or lower limbs.
The patient works as a cookie and has a significantly history of alcoholism - consumes 90 to 180ml of Officer's Choice, with frequent indulgences in "Gudumba", "Sara" and a good litre of toddy. His diet is fairly mixed and on occasions goes to bed without eating. His sexual life has taken a hit and he says he hasn't felt the same "vigour" over the last 3 months. He also frequently has to strain for defecation, which has been troubling him for 2 months now.
Finally being distressed by the state of his overall well-being, he came to the clinic for further evaluation and possible relief from all his symptoms.
Upon General examination, the patient was conscious, coherent and was well oriented to time, place and person.
Pallor was seen in the lower palpebral conjunctiva
and Quincke's pulse was seen under the fingernails
There were no signs of icterus, cyanosis, clubbing and lymphadenopathy.
The penis and scrotum were markedly enlarged. They were Transilluminant and fluctuation was seen. The patient reported mild discomfort while passing urine.


There was B/L pedal oedema seen which extends upto the knee and was pitting in nature

Vitals at the time of examination in the OP were as follows:
The patient was Afebrile, Pulse: 106 bpm(It was bounding in character) ; B.P. : 150/60mmhg
R.R. : 22 cpm. SpO2 : 97% on RA; GRBS- 116mg/dl
Systemic examination was done and the following findings were noted :
Respiratory system : B/L AE(+) , no wheeze or crepitations were heard.
The trunk:


CVS : The JVP was about 8 to 10cm above the clavicle in the sitting position. It showed prominent 'a' waves with severe Vy collapse.
The apex beat was palpable in the 6th ICS
with a diameter greater that 2.5cm and was displaced more than 12cm from the mid sternal line

On auscultation, a Grade 3 Pansystolic murmur was heard along the left sternal border and the mitral area. No diastolic murmurs were heard, no S3 was heard.
An Audicor was setup(After significant diuresis induced by medication) and and S3 of 5.2 was noted(An S3 >5 is noted in LV dysfunction usually)


GIT - P/A was soft and non tender, there were no distended veins seen over the abdomen.
The liver on percussion appeared enlarged at 19 cms and was mildly tender.

CNS - Spine was normal
speech is normal
Cranial nerves are normal
Reflexes are present and normal B/L
Cortical sensations are intact on both sides
Cerebellar functions are normal
He walks slowly and cautiously and his stride is shorter than that of a normal person.
After Admission, the following investigations were ordered :




Serology was negative for HIV, HCV antibodies and HBsAg.
CUE(pending report)
CXR



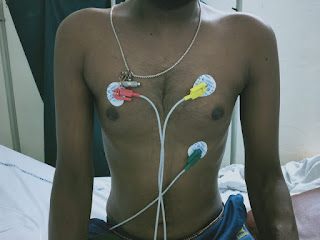
ECG


He was put on the following medication by the treating doctors :
1. Fluid restriction <1.5 litres/ day
2. Salt restriction < 6gms/ day
3. Inj. LASIX 40mg IV/BD
4. Inj. THIAMINE 2 amps in 100ml NS IV/BD
5. Inj. OPTINEURON 1 amp in 100ml NS IV/OD
Course in Hospital : From admission to the next day, there was significant diuresis (about 2l) noted.
The patients weight decreased to 57kgs from 59kgs
He reports decreased swelling in scrotum, increased exercise tolerance and improved mobility compared to before.
His Provisional diagnosis: 35 yr old Chronic alcoholic with Class 3 NYHA with high output heart failure with wet Beri Beri and B/L symmetrical axonal sensory polyneuropathy.


Comments
Post a Comment